

Infection control is one of the most important functions of every hospital. Building in an occupied hospital is a specialized job and critical responsibility.
Healthcare-associated infections pose a severe, though preventable, threat to patient safety. About 4% of hospital patients contract healthcare-associated infections each day, according to the Center for Disease Control and Prevention.
Construction can pose a risk to patients and hospital staff if precautions are not planned and executed properly. In addition to the non-negotiable process of strictly complying with hospital infection control protocol, infection control must be at the forefront of our minds in our daily operations. We treat every healthcare work zone as if our family members were next door to our site. Most of our healthcare construction team members have completed the ASHE Healthcare Construction Certificate course and actively pursue continuing education in infection control and occupied construction life safety.
As a Project Manager, I work with our field teams to ensure we are not only complying with required protocols but exceeding expectations in respecting patient comfort and protecting their safety. We outline specific standards for each project in an Infection Control Risk Assessment and Interim Life Safety Measures document (ICRA/ILSM). The three most effective measures in ensuring infection control are establishing a comprehensive ICRA and ILSM for each unique project, constructing temporary barriers and maintaining negative air in the work zone.
Prior to mobilizing every project in an occupied hospital we meet with managers from the facility, infection control, and construction departments to create an ICRA permit to determine the type and class of the project based upon the function, sensitivity and logistics for that area of the hospital. This document will dictate which infection control measures need to be implemented during construction. We post the ICRA permit and our safety logs onsite. Our ICRA plans are closely coordinated with ILSM. However, hospitals tend to be constantly changing environments, so we must be flexible when changes occur in the ICRA. When ICRA plans change all Lewis team members as well as all subcontractors meet to discuss the change to ensure everyone is aware of the state of the current work environment and the procedures that must be implemented.
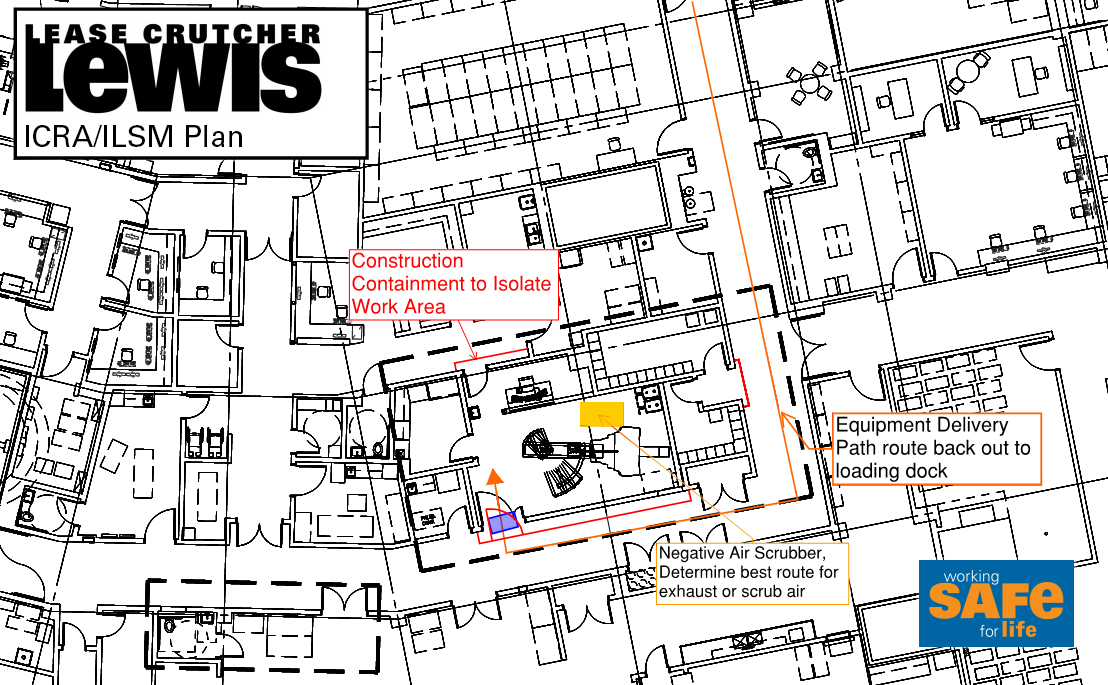
Choosing construction barriers and agreeing on employee and material access to the work zone is one of the most important steps in establishing our infection control plan. Temporary containment walls are set up to isolate our work from hospital operations. This includes installing barriers above grid ceilings and around existing utilities to keep our site fully contained. Barrier products are required to be fire-rated and range from fire retardant polyethylene (poly), metal stud framing with fire-rated core-ply (similar to posterboard), gypsum wallboard and pre-manufactured systems. Barrier types vary from one project to the next. We select barriers based on the best value for the project while also taking into account the duration, ease of cleaning, ICRA Class and noise protection required for the job.
Noise protection is a major factor to consider in supporting patient health during construction. We know that patients need a calm and quiet environment to promote a speedy recovery. We mitigate as much construction noise as possible so as not to disturb the patients’ ability to rest. I have worked on studies to determine the variation of decibels created by different tools and construction equipment, which inform how I help project teams create the best solution to meet the requested noise reduction level and target budget.
Lewis is currently using an innovative, pre-manufactured barrier by Edge Guard. This product has been used with great success on recent Lewis projects in Class IV “I”-Occupancy areas such as Emergency Departments, Operating Rooms and Central Sterile. Advantages of this product include: dust-free walls that do not require secondary containment to erect, built-in air intake/exhaust plugs and mounting for digital air pressure monitoring. They are also fire-rated and reusable, reducing waste of materials. One disadvantage is that they alone do not provide a high STC rating for noise reduction.
Another critical component in protecting patient health is developing a negative air plan to contain the debris particles released during construction. In addition to physically containing the work zone, HVAC ducts are sealed off, filtration devices are utilized and negative air pressure is monitored and continually maintained in the work zone. Ideally, the plan is to exhaust the air out to the exterior of the building. However, this is sometimes not feasible or it creates an expense larger than the project itself, requiring some creative work-around strategies. We work closely with facility managers to ensure there is a negative air plan in place prior to starting any remodel on a healthcare campus.
For those who are looking for more information on infection control best practices and procedures, I recommend the American Society for Healthcare Engineering website. It’s a fantastic resource for information and also links to local chapters and educational opportunities.
I personally enjoy supporting and contributing to the success and health of the patients in the hospitals we serve. It is fulfilling to construct and improve facilities that help so many people physically and emotionally. I take pride in mitigating any risk that construction can pose to patients’ wellbeing, as well as in maintaining an environment that will promote their recovery.